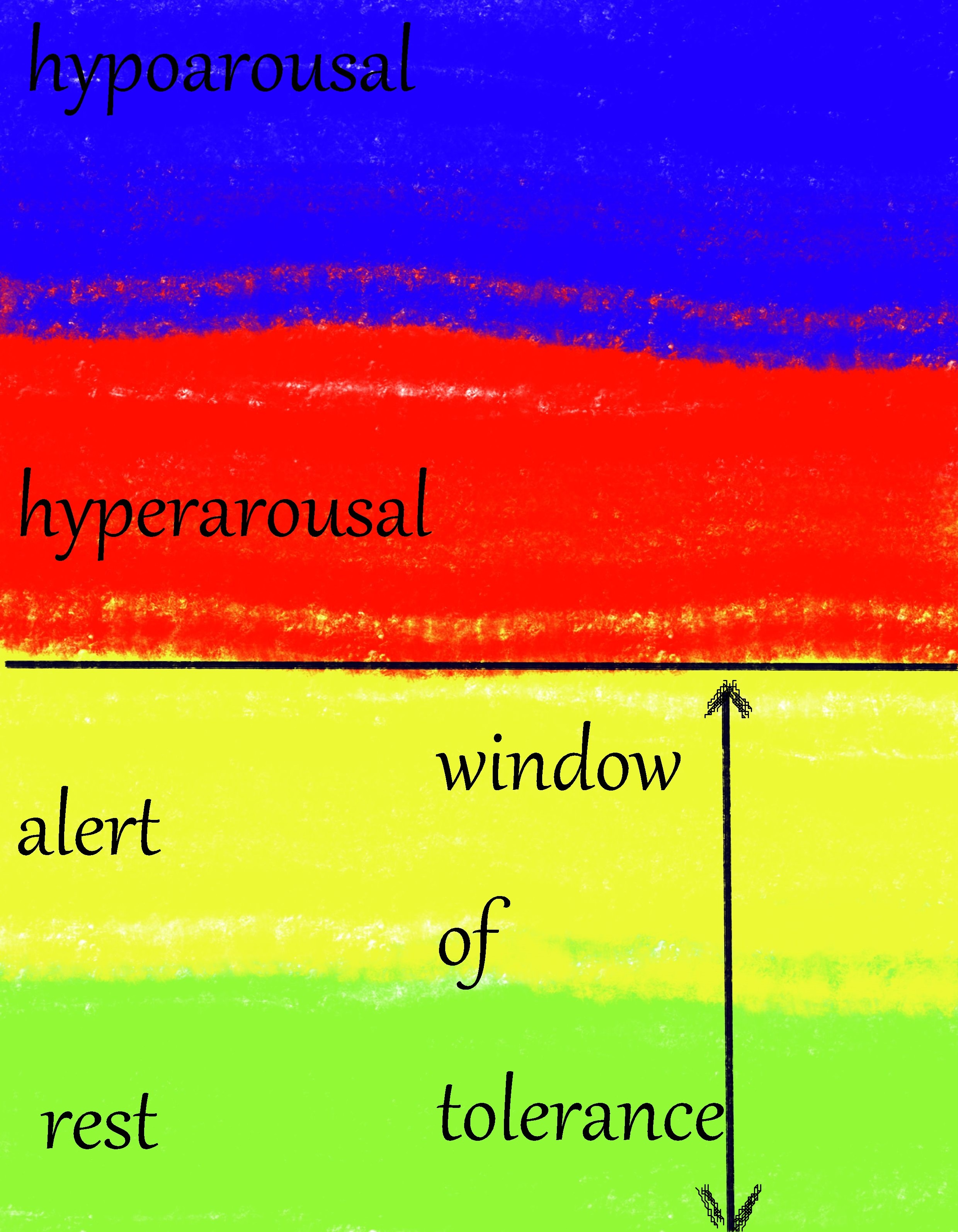
We all know the model of the Window of Tolerance. There is an area of relaxed regulation, the polyvagal theory would call it the safe&social system or ventral vagal activation and we traditionally mark it in green. We can handle a bit of activation (yellow) without getting into a difficult situation. When stress gets too much or we get triggered we might enter the red zone that stands for sympathetic activation and the flight/fight response. If that isn’t working out for us, we can enter the blue zone that is marked by freeze or dissociation and dorsal vagal activation.
The Window of Tolerance contains the green and yellow area and the goal of our therapy is to learn how to regulate ourselves within that zone and return to it after we get dysregulated. When we deal with complex trauma, we can run into several problems here. First of all, that green zone can barely exist. We never developed it because our life has never been safe and neglect led to reduced social interactions during critical times in our (brain) development. The real window of tolerance we are aiming for is tiny compared to that of people who grew up in safety.
And we rarely spend time there anyway. From early on our body did not learn to calm down and rest because that would have needed a co-regulating Other. While healthy people live most of their life on ground level within their window of tolerance we moved into the penthouse apartment and rarely leave it.
There are 2 subtypes of PTSD described in literature. One shows more hyperarousal (red zone) in response to triggers and is common in simple PTSD. The other subtype shows more hypoarousal (blue zone) in triggering situations and is more common with severe and chronic trauma experiences. For most people this is temporary and they can regulate themselves after getting triggered. Some people with early chronic trauma live with chronic dysregulation and have something called a Faux Window of Tolerance. They regulate themselves within a range of stress that is chronically elevated.
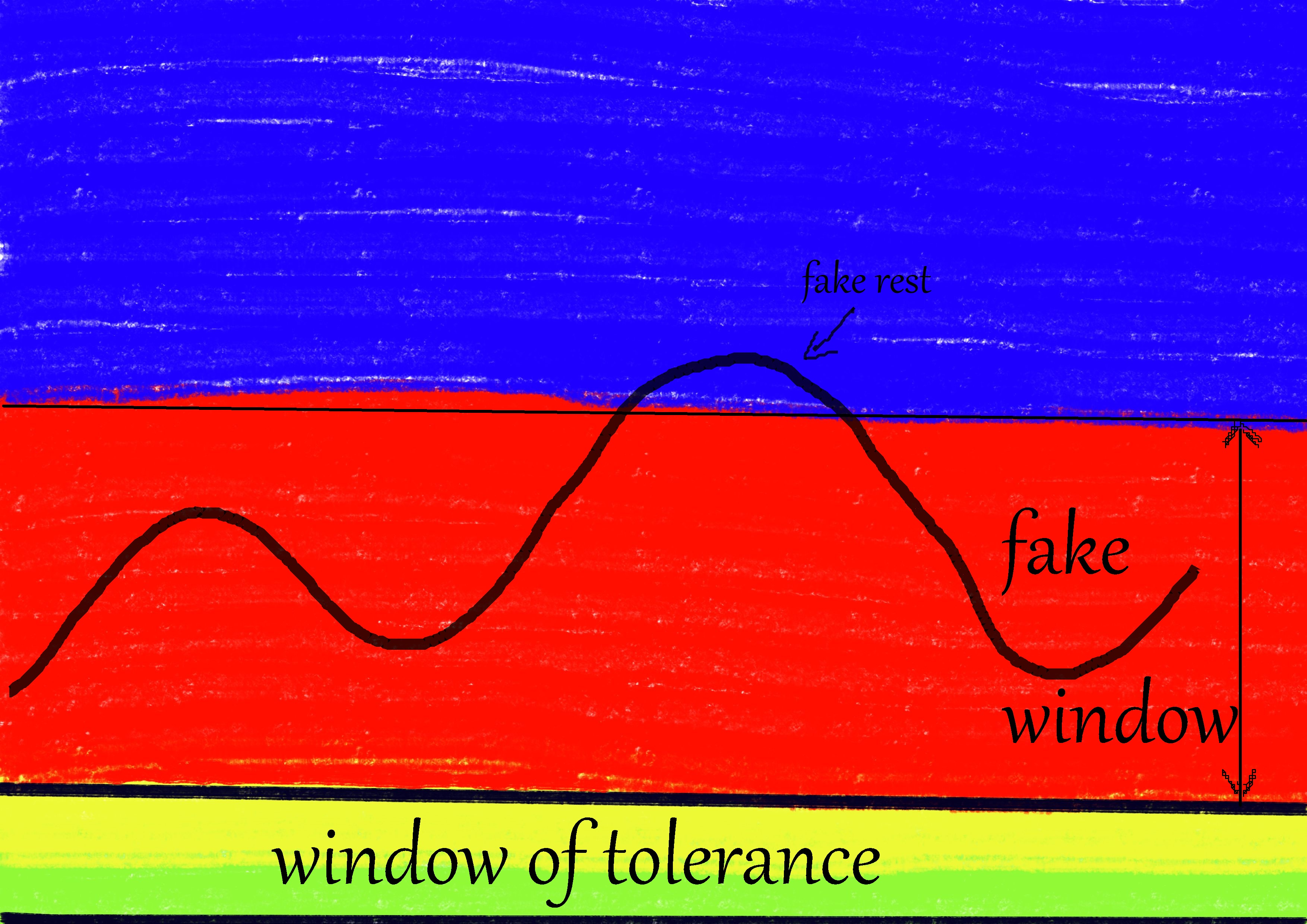
In this picture you can see what it would look like for someone who is chronically hyperaroused and experiences that as their normal zone for regulation. We never relax, don’t even get near the green zone. We just get a little less hyperaroused sometimes. When we grow still and inactive we are actually slipping into the blue zone instead of the green one as a substitute for rest. That looks like we calmed down but it is faux regulation. We just go numb or we freeze. When traumatized people of this type suddenly ‘calm down’ that is not a good sign. It is not a successful intervention or good therapy. It is not regulation. Just a different kind of out-of-control stress response. This is where intense aversive stimulation that is used in DBT can teach patients to dissociate more by pushing them up in their stress response instead of guiding them down.
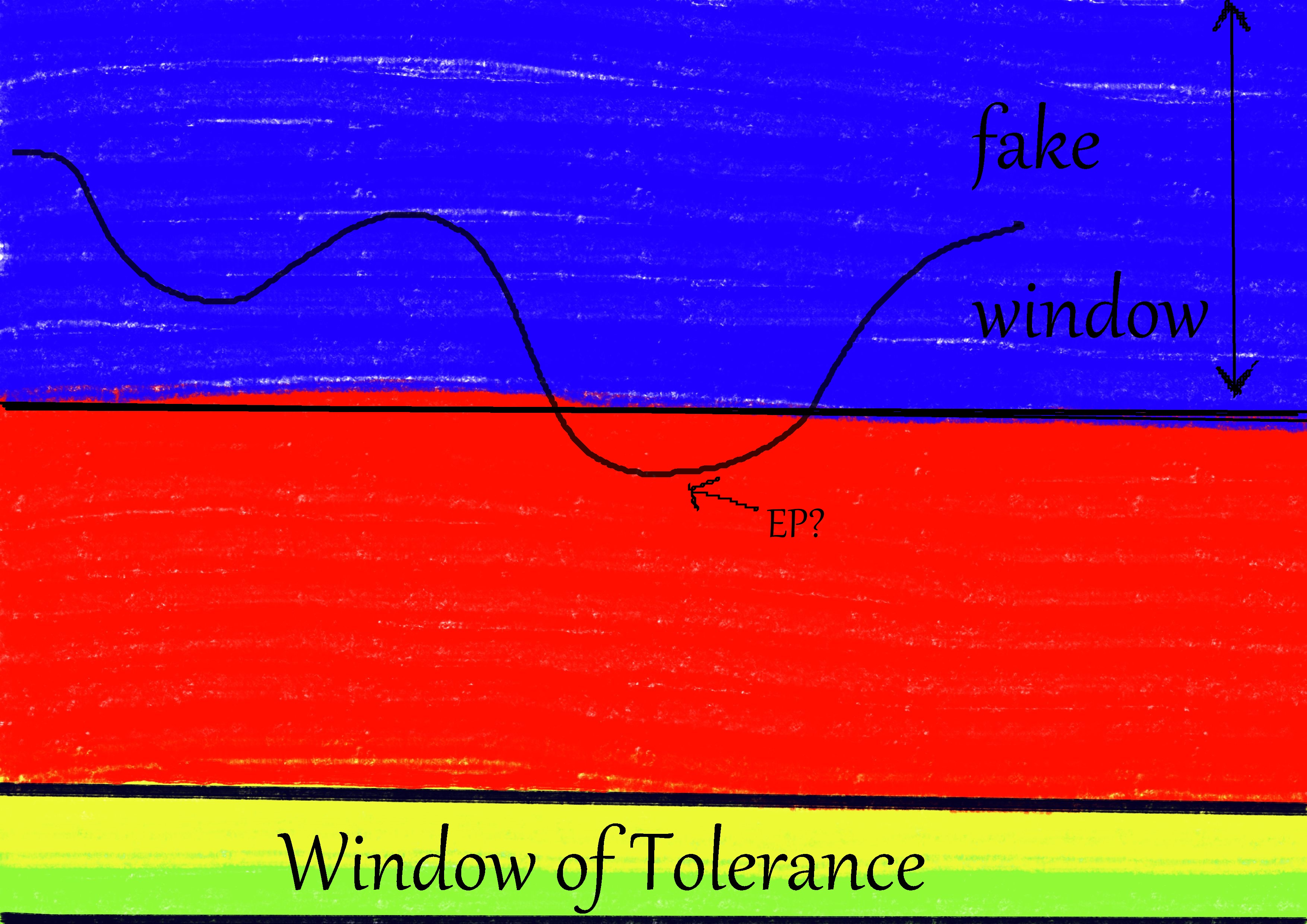
In this picture we see the same thing, just for people who live in chronic dissociation, or how it is sometimes called, functional freeze. We walk around, talk, live our life, but we are numb, chronically depressed, chronically suicidal and our field of consciousness is chronically limited because of depersonalization and derealization. Most hosts of DID systems live in this zone. We sometimes slip into hyperarousal when we become more present and aware of our experience for a while or when a hyperaroused EP shows up and then we return to our functional dissociation within our faux window of tolerance.
Seeing us calm and composed is not a sign of regulation. We present that way because we are numb and split off most of our inner experience. Not showing any intense emotions does not mean that everything is ok.
Again, intense aversive stimulation like it is used in DBT can deepen this freeze state/ the (structural) dissociation and make patients more submissive and numb. That is what happens when people seem to ‘get used’ to the aversive stimulation. In DID, hyperaroused EPs might get triggered, because they usually get activated when abuse is happening, and that isn’t regulation either. DBT skills will not miraculously bring us into the green area. We don’t even know where it is. All we know is how to split off our experiences while taking part in everyday life in a (sometimes structurally parallel) dissociated state.
In this case it is important to look for things to take away to reduce the pressure instead of trying to add even more to the situation. Don’t add stimulation, remove stressors. That can include therapists leaving the room for a moment or looking somewhere else.
When we are aware of a background of very early and chronic trauma, we must assume that the true window of tolerance is tiny and that the person regulates on higher levels within a faux window of tolerance almost exclusively. We need to double check the tools and interventions we use to ‘regulate’ because we might just make it worse. More than anything, we need to pay attention to what is really going on because what we do might just strengthen the chronic stress experience within the faux window. I hope this helps you to understand why I am so critical of DBT for chronic dysregulation. It is not an ideal approach. Knowing this model is key though.
We can learn how to live within the real window of tolerance and expand that so it is easier to stay there. Usually bodywork therapists who are specialized in develomental trauma and working with stress responses are the right people to ask for help. Psychotherapists rarely have the training to do this kind of work. You can look into techniques by Peter Levine or Kathy Kain for more information.
Liebe Theresa, Der Artikel zum falschen Window of tolerance war sehr erhellend für mich, hat mir eine neue, andere Sichtweise ermöglicht auf bisher nicht gut gelungene Interventionen ! Herzlichen Dank dafür und viele Grüße A. Schrörs
Hi. I love how you have the hypo arousal shown at the top of the window of tolerance. Is that something you’ve come up with or used from another model? I don’t understand why it’s often shown like a sandwich with hyperarousal at the top and hypoarousal at the bottom with regulated in the middle. Do people switch from regulated to hypo-aroused so quickly?
Stacking it this way is the more scientific way that is often used in body-focused trauma therapy. Since the original concept of the faux window of tolerance is from a body work background it makes sense. The other way to stack it is an old and kind of outdated way that shows how people feel (too much/not enough). Back then the idea was to balance between those so it is just right. Some still find it helpful for a short check-in where they just ask themselves if this is too much, not enough or fine. I think it is best to choose the model that fits your intuition best. None of them are able to show the full reality of what is happening. And yes, people can sometimes go into a stress response within a second. One moment they are there, the other they are gone. Not always the case but possible. They just don’t pass through a regulated state when it happens. you might be interested in the ‘polyvagal ladder’ as a fitting concept that is easy to grasp and a bit more accurate than the WoT.